
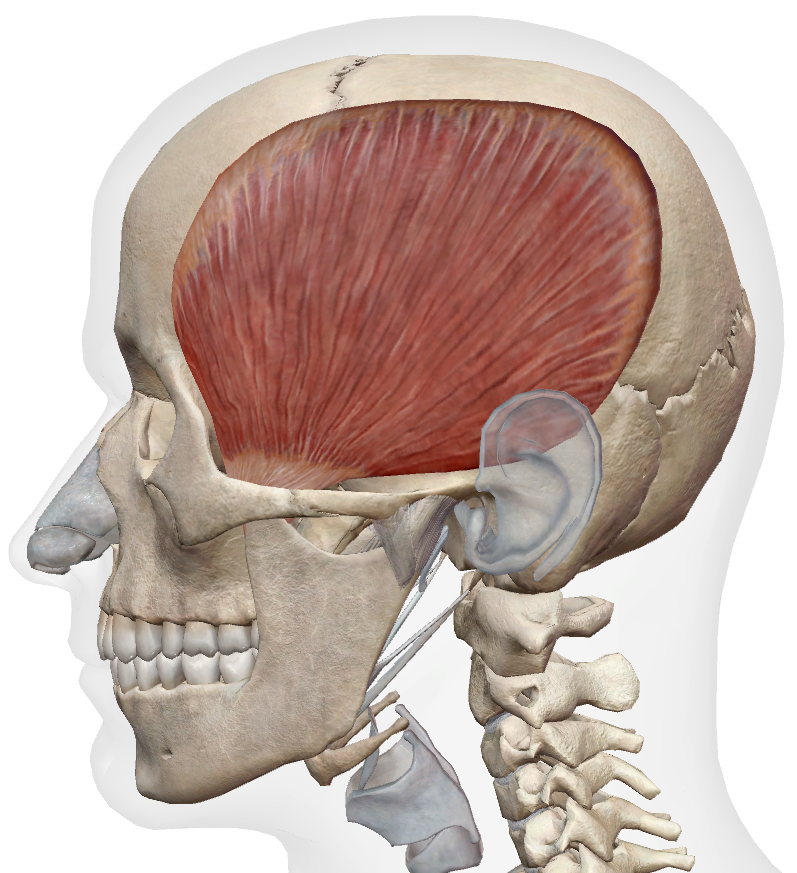
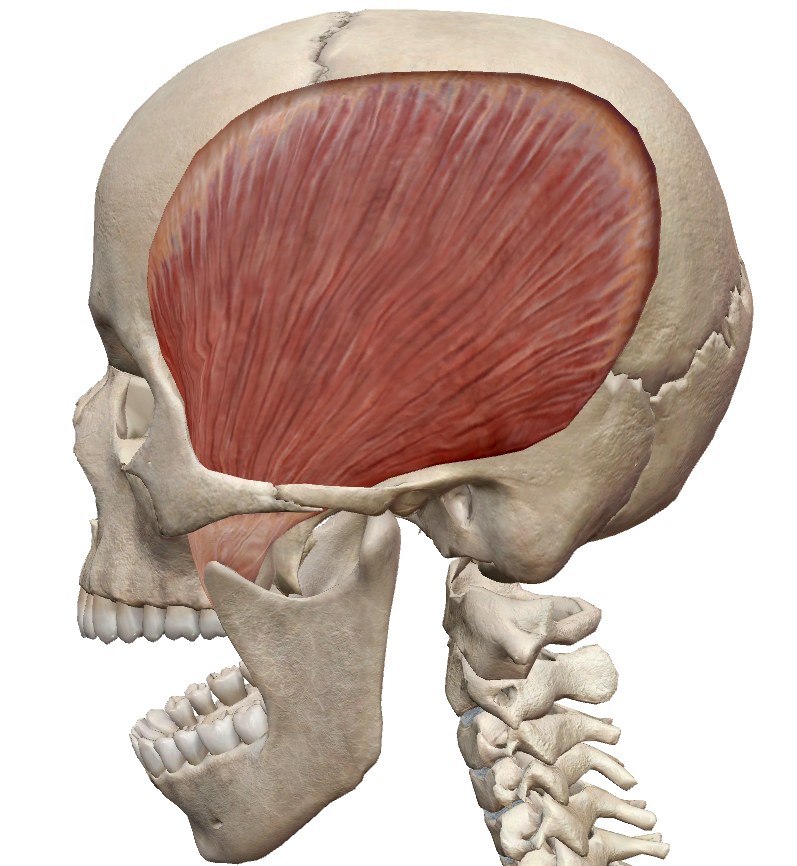
Temporalis
See Scenario 1: TMD · Scenario 2: Headaches
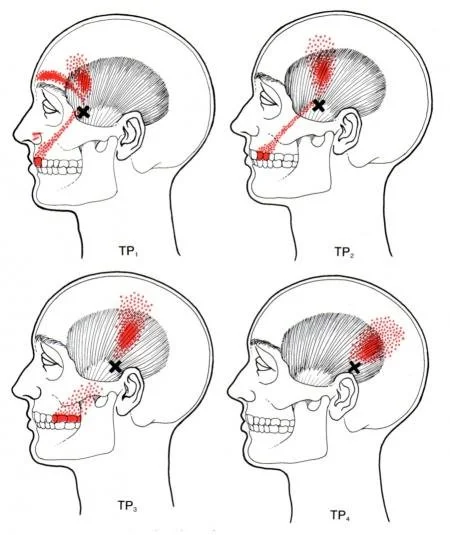
| Anterior fibres | Upper teeth, eyebrow — often mistaken for dental pain |
| Middle & posterior fibres | Temple, side of head, behind the eye, retro-orbital pain |
Client position: Supine (preferred) or seated. Jaw fully relaxed — teeth slightly apart, lips lightly touching.
Client communication: “I’m going to work on the muscles along the side of your head and temple. It can be quite tender, especially if you’ve been clenching. Breathe normally and let me know if the pressure is too strong.”
Locate & confirm: Place fingertips across the temporal fossa. Ask client to clench gently — the muscle fans out and hardens under your fingers. Ask them to relax and confirm softening. This clenching and release helps you map the full muscle boundary before working into it.
Anterior fibres
Palpate: Vertical fibres above the zygomatic arch toward the corner of the eye. Most commonly hypertonic in clenchers.
What to feel for: Taut bands and point tenderness that reproduce upper molar or eyebrow pain. This is the most clinically significant region for dental pain referral.
Middle & posterior fibres
Palpate: Middle fibres run obliquely across the temporal fossa. Posterior fibres are more horizontal, toward the occiput. Palpate both sides and compare.
What to feel for: Diffuse hypertonicity across the middle belly (common in chronic bruxers), deeper tenderness in the posterior fibres that reproduces temple or retro-orbital pain, asymmetry between sides.
Client supine, jaw relaxed. Pin the temporal belly with fingertips or flat thumb across the fibre direction. Work each region in sequence: anterior, middle, posterior. At each pin, ask client to open the jaw slowly and fully, then return to neutral. Maintain pin pressure throughout. Repeat 4–6 cycles per section. Adjust pin location between passes to cover the full belly.
Work systematically through anterior, middle, and posterior fibres. Sustained pressure on identified taut bands or nodules — firm but tolerable. Hold 60–90 seconds or until softening. Anterior fibre referral to the upper teeth during treatment is common and diagnostically useful — confirm it reproduces familiar symptoms. Maximum 2–3 trigger points per session.
The temporalis is a jaw closer. PIR is the appropriate approach: resisted jaw closing at end of opening range produces post-isometric relaxation and passive gain in opening.
Client supine. Bring the jaw to end of comfortable opening range. Place a cupped hand under the chin. Ask the client to close the jaw gently against your upward resistance (10–20% effort). Hold 5–7 seconds. Relax — jaw drops open passively, do not force it. Repeat 3–5 times.
Cross-fibre strokes at the inferior attachment on the coronoid process. Firm and precise — 30–60 seconds. Not a primary technique; use when the attachment is specifically reactive and belly work alone is insufficient.
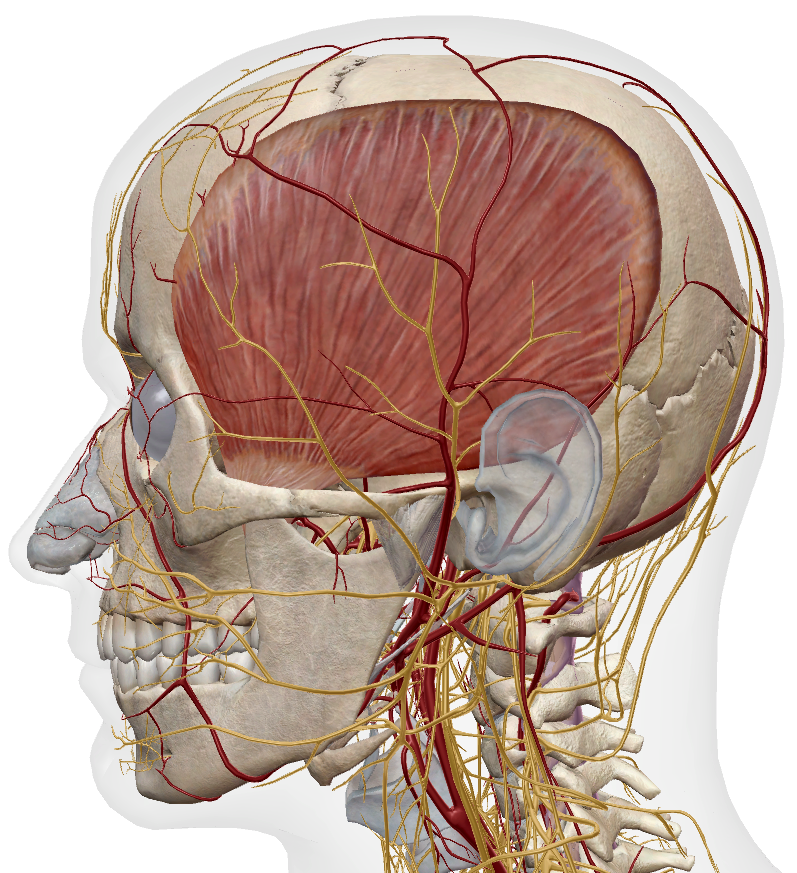
Superficial temporal artery: Runs through the temporal fossa — palpable as a pulsating vessel, often visible in thin clients. Avoid sustained direct pressure over this structure. Work around it, not on it. If the client reports a pulsating sensation under your fingers, reposition immediately.
Pressure threshold: The temporalis can be extremely tender in clients with active headaches or chronic clenching. Start very light. Build pressure gradually and confirm tolerance before increasing depth. Do not assume the level of pressure tolerated on one region applies to the next.
Headache provocation: If palpation or technique provokes or worsens a headache during treatment — reduce pressure immediately and reassess before continuing. Do not push through a technique-provoked headache.
Technique limit: If jaw symptoms worsen, temporal pain spreads, or the client reports sharp or catching pain during treatment — stop and reassess. Do not push through sharp pain.