
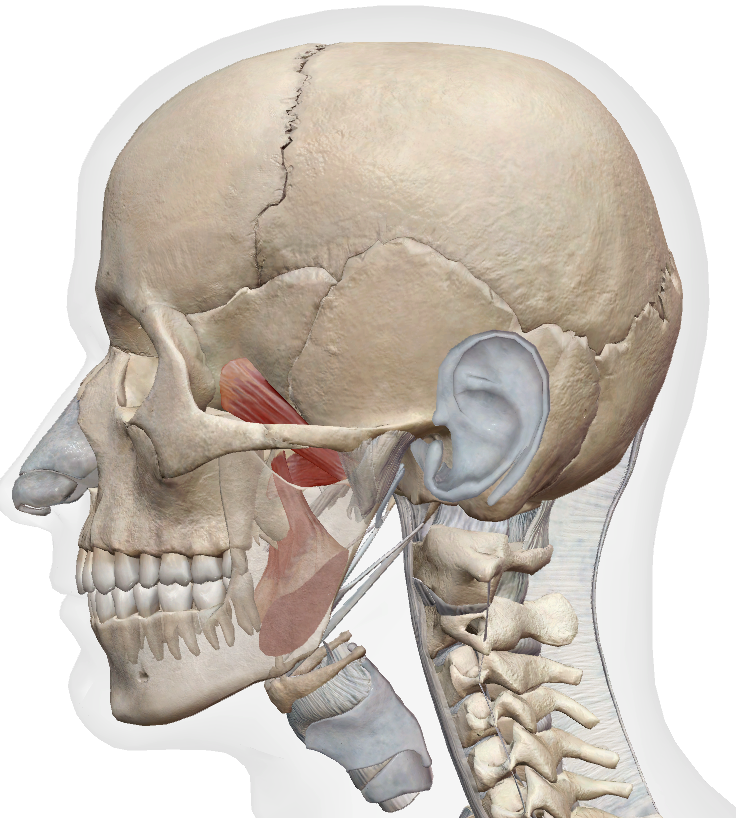
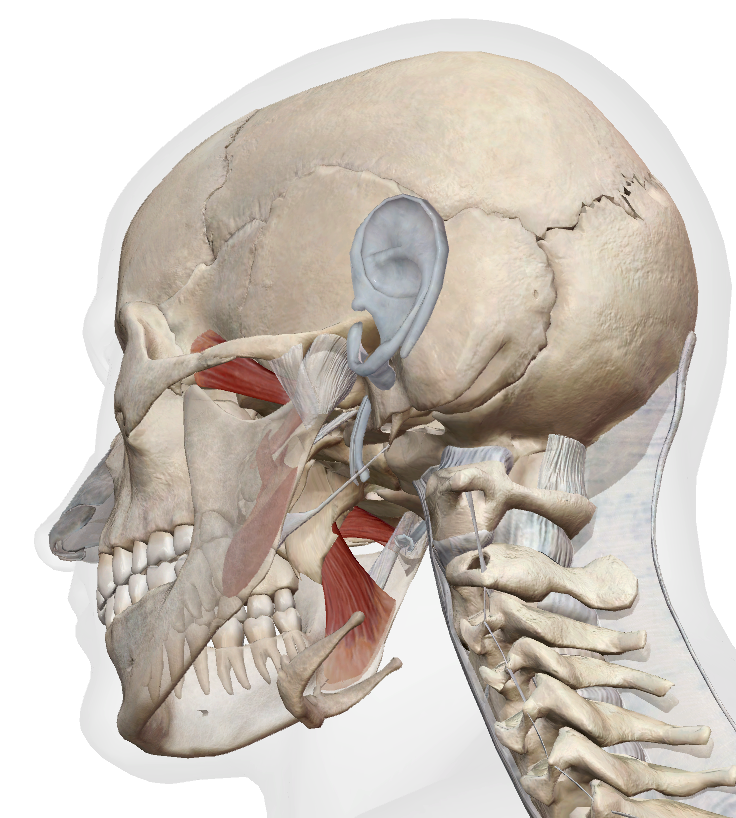
Pterygoids
Medial & Lateral · See Scenario 1: TMD
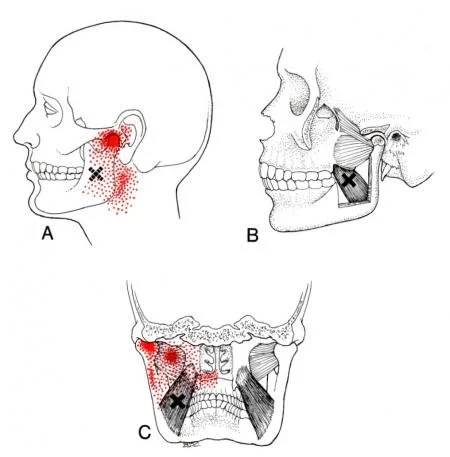
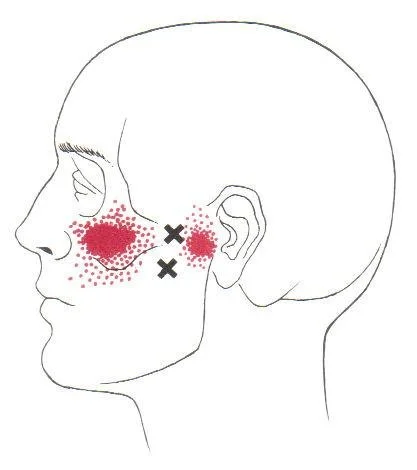
| Medial pterygoid | Pain inside the mouth, throat, and below the ear — can mimic ear pain, throat pain, or a sense of fullness in the ear |
| Lateral pterygoid | Deep pain in the TMJ region and cheek; can refer into the maxillary sinus area — can mimic sinusitis |
Client position: Supine, head in neutral. Pillow removed or flat. Therapist seated at head of table.
Client communication: “I’m going to work inside your mouth with a gloved finger. You’ll feel pressure, and it may be quite tender, especially on the side that’s been giving you trouble. Breathe slowly through your nose. If the pressure becomes too strong, raise your hand and I’ll ease off straight away.”
Medial pterygoid
Locate & confirm: Glove on. Slide your index finger along the inner surface of the lower molars to the retromolar fossa — just behind the last molar. Press laterally against the medial surface of the ramus.
What to feel for: Significant tenderness, often disproportionate to the pressure used. Reproduction of deep jaw ache, throat pain, or ear fullness confirms the trigger point.
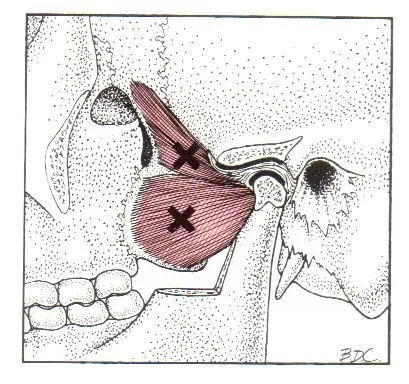
Lateral pterygoid
Locate & confirm: Glove on. Slide your index finger along the inner surface of the upper molars to the upper retromolar area — past the last molar. Angle the finger superiorly and medially into the infratemporal space. Ask the client to perform a small jaw protrusion — the inferior head contracts, confirming placement.
What to feel for: Deep, sharp tenderness. Reproduction of TMJ pain or cheek pain confirms involvement. This area is frequently exquisitely tender in clients with disc displacement or deviation on opening.
Medial: Gloved index finger contacts the medial pterygoid at the retromolar fossa, pressing laterally against the ramus. Ask the client to open the jaw slowly and fully, then return to neutral. Repeat 4–6 cycles. Adjust pin location between sets to cover the full belly.
Lateral: Gloved index finger contacts the lateral pterygoid in the infratemporal space, superior to the last upper molar. Ask the client to deviate the jaw slowly to the ipsilateral side (same side as the pin), then return to neutral. Repeat 4–6 cycles.
Medial: Sustained pressure to the identified trigger point at the retromolar fossa, pressing laterally against the ramus. Hold 60–90 seconds or until referred pain reduces. Client breathes through the nose throughout.
Lateral: Sustained pressure in the infratemporal space. Hold 60–90 seconds. Do not increase pressure if strong referred pain is present — maintain and wait for release. Client breathes through the nose.
Medial — PIR: Client supine. Cupped hand placed under the chin. Ask client to close the jaw against gentle upward resistance (10–20% effort). Hold 5–7 seconds. Relax — jaw drops open passively, do not force it. Repeat 3–5 times.
Lateral — resisted opening: Hand placed lightly at the chin. Ask client to open the jaw, or deviate laterally to the ipsilateral side, against gentle resistance. Hold 5–7 seconds. On release, mobility improves passively. Repeat 3–5 times. PIR is not applicable here — the lateral pterygoid opens the jaw, so resisted opening is the correct approach.
Technique not indicated for either muscle. Intraoral and deep external access make effective cross-fibre friction delivery impractical. Sustained TPT pressure is the appropriate alternative.
Intraoral consent: Any intraoral technique requires explicit informed consent before every session — not just on intake. Some clients will decline; this must be respected without pressure. Never proceed without clear agreement. Gloves required for all intraoral contact. Fingernails trimmed short.
Sensitive structures — medial pterygoid: Lingual nerve and inferior alveolar nerve run adjacent to the medial pterygoid intraorally. Avoid aggressive probing. Check for dental work, crowns, or sensitivity before intraoral contact. Any shooting sensation to the lower teeth or lip — adjust position immediately.
Sensitive structures — lateral pterygoid: Middle meningeal artery and maxillary artery branches are present in the infratemporal fossa. Approach is always controlled, steady pressure — never probing. Do not attempt direct external palpation as a primary method for the lateral pterygoid.
Technique limit: If symptoms worsen, joint noise increases, or the client reports sharp catching during treatment — stop and reassess. Do not push through sharp joint-adjacent pain.